|
|
Release Notes:
Measure Information Form Version 2010B Measure Information Form Numerator Statement: The number of patients who were screened for alcohol use using a validated screening questionnaire for unhealthy drinking.
Risk Adjustment: No.
Data Collection Approach: Retrospective data sources for required data elements include administrative data and medical records. Some hospitals may prefer to gather data concurrently by identifying patients in the population of interest. This approach provides opportunities for improvement at the point of care/service. However, complete documentation includes the principal and other ICD-9-CM diagnoses which require retrospective data entry.
Data Accuracy: Data accuracy is enhanced when all definitions are used without modification. The data dictionary should be referenced for definitions and abstraction notes when questions arise during data collection.
Measure Analysis Suggestions: Hospitals may wish to analyze data to show the rate of those who were actually screened for alcohol use status, subtracting those that refused the screen.
Sampling: Yes. For additional information see the Population and Sampling Specifications section
Data Reported As: Aggregate rate generated from count data reported as a proportion.
Selected References:
1. The National Quality Forum, National Voluntary Consensus Standards for the Treatment of Substance Use Conditions: Evidence-Based Treatment Practices; A Consensus Report; 2007.
2. Harwood, HJ, 2000. Updating Estimates of the Economic Costs of Alcohol Abuse in the United States. National Institute on Alcohol Abuse and Alcoholism. Available at: http://pubs.niaaa.nih.gov/publications/economic-2000, Office of National Drug Control Policy. The Economic Costs of Drug Abuse in the United States: 19922002. Washington, DC: Executive Office of the President (Publication No. 207303), 2004.
3. Mokdad AH, Marks JS, Stroup DS, Geberding JL. Actual Causes of Death in the United States, 2000. JAMA 2004;291:128-1245.
4. Madras BK, Compton WM, Avula D, Stegbauer T, Stein JB, Clark HW. Screening, Brief Intervention, Referral to Treatment (SBIRT) for Illicit Drug and Alcohol Use at Multiple Health Care Sites: Comparison at Intake and Six Months Later. Drug Alcohol Depend. 2009;99:280-295.
5. Substance Abuse and Mental Health Services Administration. Results from the 2006 National Survey on Drug Use and Health: National Findings. Office of Applied Studies, NSDUH Series H-32, DHHS Publication No. SMA 07-4293. Rockville, 2007.
6. National Institute on Alcohol Abuse and Alcoholism (NIAAA), Helping Patients Who Drink Too Much: A Clinicians Guide, 2005 Edition, Rockville, MD.
7. Fleming MF, Mundt MP, French MT, Manwell LB, Stauffacher EA, Barry KL. Brief physician advice for problem drinkers: Long-term efficacy and cost-benefit analysis. Alcohol Clin Exp Res. 2002 Jan;26(1):36-43.
8. Gentilello LM, Ebel BE, Wickizer TM, Salkever DS Rivera FP. Alcohol interventions for trauma patients treated in emergency departments and hospitals: A cost benefit analysis. Ann Surg. 2005 Apr;241(4):541-50.
9. Gentilello LM, Villaveces A, Ries RR, Nason KS, Daranciang E, Donovan DM Copass M, Jurkovich GJ Rivara FP. Detection of acute alcohol intoxication and chronic alcohol dependence by trauma center staff. J Trauma. 1999 Dec;47(6):1131-5; discussion 1135-9.
10. Bernstein J, Bernstein E, Tassiopoulos K, Heren T, Levenson S, Hingson R. Brief motivational interventions at a clinic visit reduces cocaine and heroin use. Drug Alcohol Depend. 2005 Jan 7;77(1):49-59.
11. Madras BK, Compton WM, Avula D, Stegbauer T, Stein JB, Clark HW. Screening, brief interventions, referral to treatment (SBIRT) for illicit drug and alcohol use at multiple healthcare sites: Comparison at intake and 6 months later. Drug Alcohol Depend. 2009 Jan 1;99(1-3):280-95. Epub 2008 Oct 16.
12. Rehm J, Room R, Graham K, Monteiro M, Gmel G, Sempos CT. The relationship of average volume of alcohol consumption and patterns of drinking to burden of disease: An overview. Addiction. 2003 Sep;98(9):1209-28.
13. Smothers BA, Yahr HT, Sinclair MD. (). Prevalence of current DSM-IV alcohol use disorders in short-stay, general hospital admissions, United States, 1994. Arch Intern Med. 2003 Mar 24;163(6):713-9.
14. Smothers BA, Yahr HT, Ruhl CE. Detection of alcohol use disorders in general hospital admissions in the United States. Arch Intern Med. 2004 Apr 12;164(7):749-56.
15. CPT Assistant. Coding communication: Screening and brief intervention (SBI) for alcohol and substance abuse (other than tobacco). May 2008;18(5).
Measure Algorithm:
Included Populations:Denominator Statement: The number of hospitalized inpatients, 18 years of age and older Included Populations: Not applicable Excluded Populations: 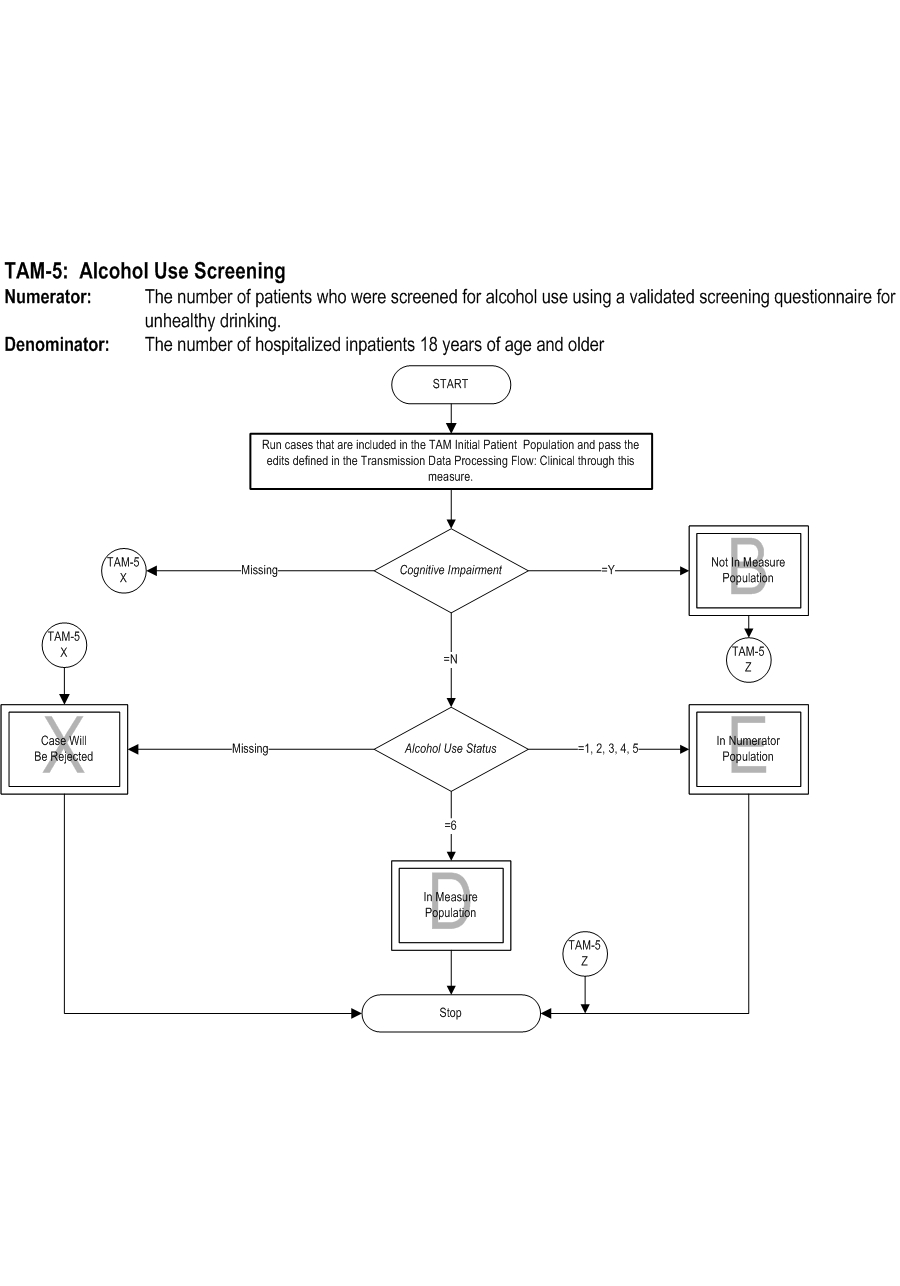
 Attach file Attach file
|
|||
Questions? Ask Question to Joint Commission staff
Copyright © 2010 by The Joint Commission.