|
|
Release Notes:
Measure Information Form Version 2010B Measure Information Form Numerator Statement: The number of patients who were screened for tobacco use status
Risk Adjustment: No.
Data Collection Approach: Retrospective data sources for required data elements include administrative data and, if applicable, medical record documents. Some hospitals may prefer to gather data concurrently by identifying patients in the population of interest. This approach provides opportunities for improvement at the point of care/serice. However, complete documentation includes the principal and other ICD-9-CM diagnoses which require retrospective data entry.
Data Accuracy: Data accuracy is enhanced when all definitions are used without modification. The data dictionary should be referenced for definitions and abstraction notes when questions arise during data collection.
Measure Analysis Suggestions: Hospitals may wish to analyze data to show the rate of those who were actually screened for tobacco use status, subtracting those that refused the screen.
Sampling: Yes. For additional information see the Population and Sampling Specifications section
Data Reported As: Aggregate rate generated from count data reported as a proportion.
Selected References:
1. Centers for Disease Control and Prevention. Annual Smoking-Attributable Mortality, Years of Potential Life Lost, and Productivity LossesUnited States, 2000-2004. Morbidity and Mortality Weekly Report (MMWR) 2008. 57(45): 1226-1228. Available at: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5745a3.htm-/.
2. McGinnis JM, Foege WH. Actual causes of death in the United States. JAMA 1993 Nov 10;270(18):2207-12.
3. U.S. Department of Health and Human Services. The health consequences of smoking: a report of the Surgeon General. Atlanta, GA, U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, 2004.
4. Centers for Disease Control and Prevention. Best Practices for Comprehensive Tobacco Control Programs2007. Atlanta, GA, Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, 2007.
5. U.S. Department of Health and Human Services. Reducing tobacco use: a report of the Surgeon General. Atlanta, GA, U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, 2000.
6. Baumeister SE, Schumann A, Meyer C, et al. Effects of smoking cessation on health care use: is elevated risk of hospitalization among former smokers attributable to smoking-related morbidity? Drug Alcohol Depend. 2007 May 11;88(2-3):197-203. Epub 2006 Nov 21.
7. Lightwood JM. The economics of smoking and cardiovascular disease. Prog Cardiovasc Dis. 2003 Jul-Aug;46(1):39-78.
8. Lightwood JM, Glantz SA. Short-term economic and health benefits of smoking cessation: myocardial infarction and stroke. Circulation. 1997 Aug 19;96 (4):1089-96.
9. Rigotti NA, Munafo MR, Stead LF. Smoking cessation interventions for hospitalized smokers: a systematic review. Arch Intern Med. 2008 Oct 13;168 (18):1950-60.
Measure Algorithm:
Included Populations:Denominator Statement: The number of hospitalized inpatients 18 years of age and older Included Populations: Not applicable Excluded Populations: 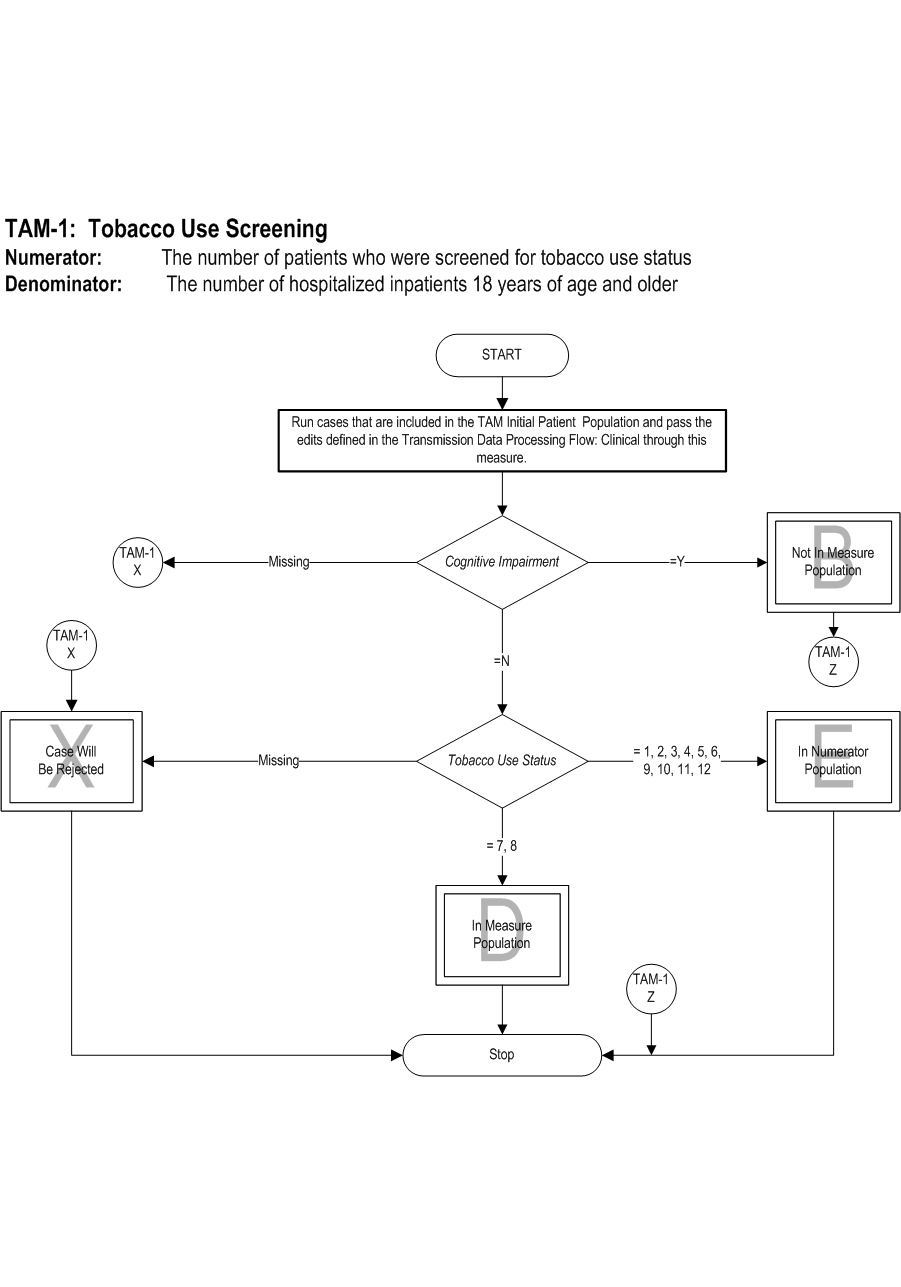
 Attach file Attach file
|
|||
Questions? Ask Question to Joint Commission staff
Copyright © 2010 by The Joint Commission.