Measure Information Form
Version 2023A
Measure Information Form
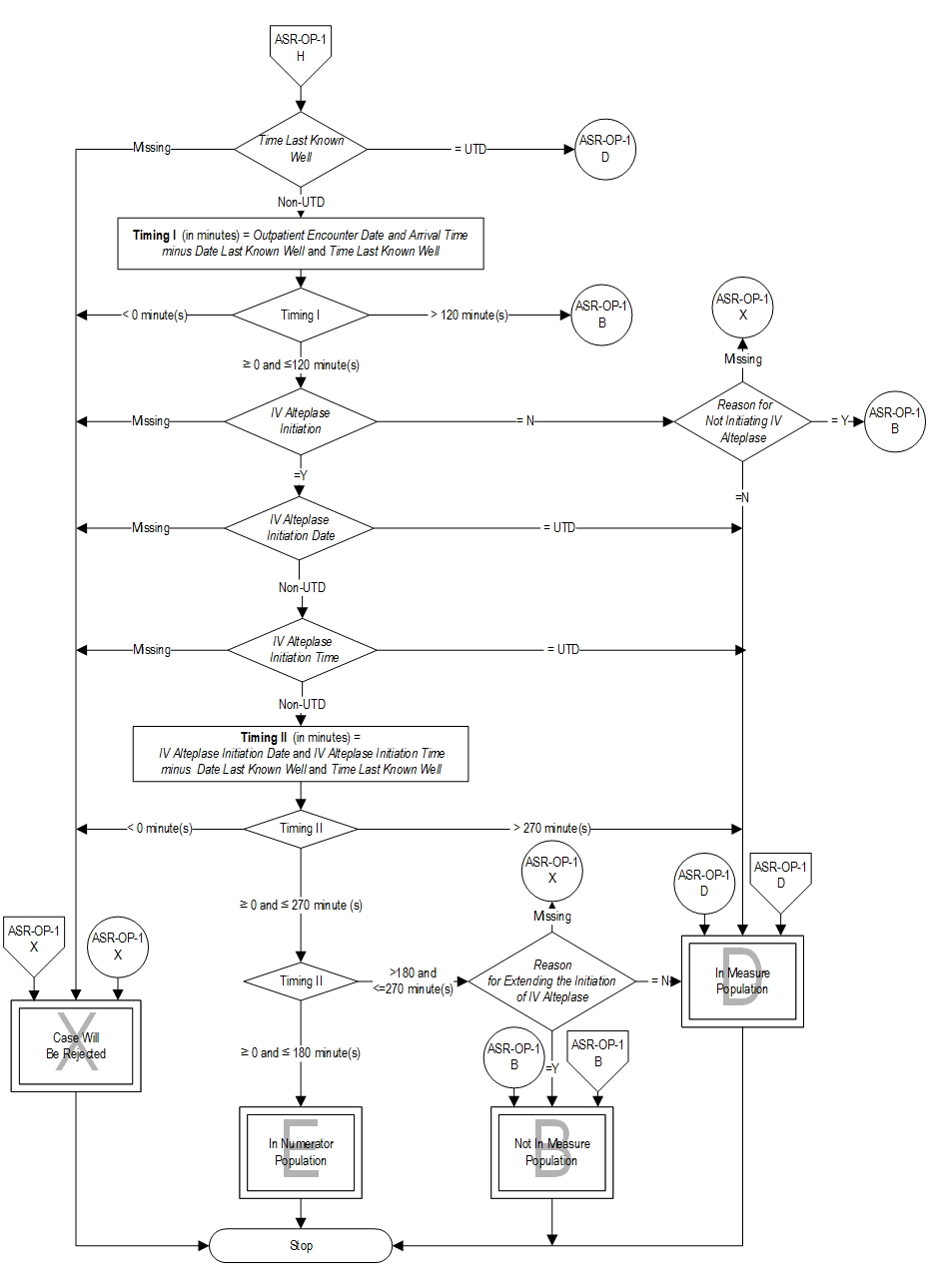
The European Cooperative Acute Stroke Study (ECASS) III trial indicated that intravenous thrombolytic therapy (tPA; rtPA) can be given safely to, and can improve outcomes for, carefully selected patients treated 3 to 4.5 hours after stroke; however, as the NINDS investigators concluded, the earlier that IV thrombolytic therapy is initiated, the better the patient outcome. Therefore, the target for IV alteplase initiation remains within 3 hours of time last known well. The administration of IV alteplase beyond 3 hours of stroke symptom onset has not been FDA approved.
Although the benefit of IV alteplase has been well established, only a minority of patients with acute ischemic stroke actually receive this medication across the United States. Recent recommendations from the American Heart Association/American Stroke Association and FDA remove or make less specific many previous contraindications and warnings for therapy.
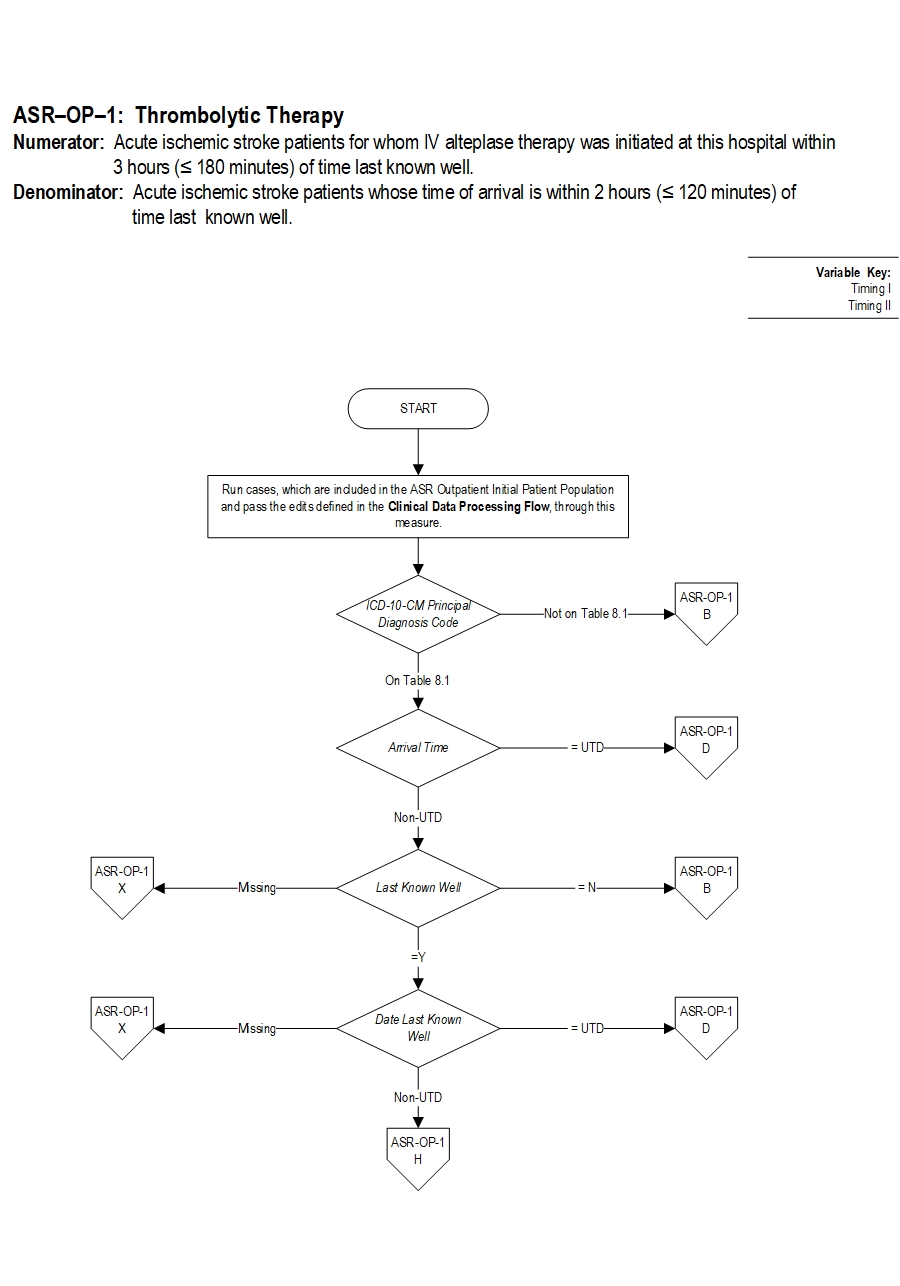
Type Of Measure: Process Improvement Noted As: Increase in the rateIncluded Populations: Not applicable Excluded Populations: None Data Elements:Denominator Statement: Acute ischemic stroke patients whose time of arrival is within 2 hours (< 120 min.) of time last known well
Included Populations:Excluded Populations:
- Patients with an ICD-10-CM Principal Diagnosis Code for acute ischemic stroke as defined in Appendix A, Table 8.1, AND
- An E/M Code for emergency department encounter as defined in Appendix A, Table 1.0
Data Elements:
- Patients less than 18 years of age
- Time Last Known Well to arrival in ED > 2 hours
- Patients with a documented Reason for Extending the Initiation of IV Alteplase
- Patients with a documented Reason for Not Initiating IV Alteplase
- H., R. Adams, G. Del Zoppo, L. B. Goldstein, Association Stroke Council of the American Heart, and Association American Stroke. "Guidelines for the Early Management of Patients with Ischemic Stroke: 2005 Guidelines Update a Scientific Statement from the Stroke Council of the American Heart Association/American Stroke Association." [In eng]. Stroke 36, no. 4 (Apr 2005): 916-23.
- Adams, H. P., Jr., G. del Zoppo, M. J. Alberts, D. L. Bhatt, L. Brass, A. Furlan, R. L. Grubb, et al. "Guidelines for the Early Management of Adults with Ischemic Stroke: A Guideline from the American Heart Association/American Stroke Association Stroke Council, Clinical Cardiology Council, Cardiovascular Radiology and Intervention Council, and the Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary Working Groups: The American Academy of Neurology Affirms the Value of This Guideline as an Educational Tool for Neurologists." [In eng]. Stroke 38, no. 5 (May 2007): 1655-711.
- Albers, G. W., P. Amarenco, J. D. Easton, R. L. Sacco, and P. Teal. "Antithrombotic and Thrombolytic Therapy for Ischemic Stroke: The Seventh Accp Conference on Antithrombotic and Thrombolytic Therapy." [In eng]. Chest 126, no. 3 Suppl (Sep 2004): 483S-512S.
- Brott, T. G., W. M. Clark, S. C. Fagan, J. C. Grotta, L. N. Hopkins, E. C. Jauch, R. E. Latchaw, and S. Starkman. "Stroke: The First Hours. Guidelines for Acute Treatment." National Stroke Association (NSA) (2000).
- Centers for Disease Control and Prevention. "Prevalence and Most Common Causes of Disability among Adults--United States, 2005." [In eng]. MMWR Morb Mortal Wkly Rep 58, no. 16 (May 1 2009): 421-6.
- Del Zoppo, G. J., J. L. Saver, E. C. Jauch, H. P. Adams, Jr., and Council American Heart Association Stroke. "Expansion of the Time Window for Treatment of Acute Ischemic Stroke with Intravenous Tissue Plasminogen Activator: A Science Advisory from the American Heart Association/American Stroke Association." [In eng]. Stroke 40, no. 8 (Aug 2009): 2945-8.
- Demaerschalk, B. M., D. O. Kleindorfer, O. M. Adeoye, A. M. Demchuk, et. al., on behalf of the American Heart Association Stroke Council and Council on Epidemiology and Prevention. “Scientific Rationale for the Inclusion and Exclusion Criteria for Intravenous Alteplase in Acute Ischemic Stroke: As Statement for Healthcare Professionals From the American Heart Association/American Stroke Association.” [In eng]. Stroke, no. 47 (Feb 2016): 581-641.
- "Diagnosis and Initial Treatment of Ischemic Stroke." Institute for Clinical Systems Improvement (2001).
- Fagan, S. C., L. B. Morgenstern, A. Petitta, R. E. Ward, B. C. Tilley, J. R. Marler, S. R. Levine, et al. "Cost-Effectiveness of Tissue Plasminogen Activator for Acute Ischemic Stroke. Ninds Rt-Pa Stroke Study Group." [In eng]. Neurology 50, no. 4 (Apr 1998): 883-90.
- Guyatt, G. H., E. A. Akl, M. Crowther, D. D. Gutterman, H. J. Schuunemann, Therapy American College of Chest Physicians Antithrombotic, and Panel Prevention of Thrombosis. "Executive Summary: Antithrombotic Therapy and Prevention of Thrombosis, 9th Ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines." [In eng]. Chest 141, no. 2 Suppl (Feb 2012): 7S-47S.
- Hacke, W., G. Donnan, C. Fieschi, M. Kaste, R. von Kummer, J. P. Broderick, T. Brott, et al. "Association of Outcome with Early Stroke Treatment: Pooled Analysis of Atlantis, Ecass, and Ninds Rt-Pa Stroke Trials." [In eng]. Lancet 363, no. 9411 (Mar 6 2004): 768-74.
- Hacke, W., M. Kaste, E. Bluhmki, M. Brozman, A. Davalos, D. Guidetti, V. Larrue, et al. "Thrombolysis with Alteplase 3 to 4.5 Hours after Acute Ischemic Stroke." [In eng]. N Engl J Med 359, no. 13 (Sep 25 2008): 1317-29.
- Hacke, W., M. Kaste, C. Fieschi, D. Toni, E. Lesaffre, R. von Kummer, G. Boysen, et al. "Intravenous Thrombolysis with Recombinant Tissue Plasminogen Activator for Acute Hemispheric Stroke. The European Cooperative Acute Stroke Study (Ecass)." [In eng]. JAMA 274, no. 13 (Oct 4 1995): 1017-25.
- Jauch, E. C., J. L. Saver, H. P. Adams, Jr., A. Bruno, J. J. Connors, B. M. Demaerschalk, P. Khatri, et al. "Guidelines for the Early Management of Patients with Acute Ischemic Stroke: A Guideline for Healthcare Professionals from the American Heart Association/American Stroke Association." [In Eng]. Stroke (Jan 31 2013).
- Kwiatkowski, T. G., R. B. Libman, M. Frankel, B. C. Tilley, L. B. Morgenstern, M. Lu, J. P. Broderick, et al. "Effects of Tissue Plasminogen Activator for Acute Ischemic Stroke at One Year. National Institute of Neurological Disorders and Stroke Recombinant Tissue Plasminogen Activator Stroke Study Group." [In eng]. N Engl J Med 340, no. 23 (Jun 10 1999): 1781-7.
- "Management of Patients with Stroke: Rehabilitation, Prevention and Management of Complications, and Discharge Planning. A National Clinical Guideline.". http://www.sign.ac.uk/guidelines/fulltext/118/.
- Marler, J. R., B. C. Tilley, M. Lu, T. G. Brott, P. C. Lyden, J. C. Grotta, J. P. Broderick, et al. "Early Stroke Treatment Associated with Better Outcome: The Ninds Rt-Pa Stroke Study." [In eng]. Neurology 55, no. 11 (Dec 12 2000): 1649-55.
- Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, Biller J, et al; on behalf of the American Heart Association Stroke Council. 2018 Guidelines for the Early Management of Patients with Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke. 2018 Jan;49:e18-e25.
- Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, Biller J, et al. Guidelines for the Early Management of Patients with Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke. A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke. 2019 Dec;50(12):e344-e418.
- Roger, V. L., A. S. Go, D. M. Lloyd-Jones, E. J. Benjamin, J. D. Berry, W. B. Borden, D. M. Bravata, et al. "Heart Disease and Stroke Statistics--2012 Update: A Report from the American Heart Association." [In eng]. Circulation 125, no. 1 (Jan 3 2012): e2-e220.
- Sacco, R. L., R. Adams, G. Albers, M. J. Alberts, O. Benavente, K. Furie, L. B. Goldstein, et al. "Guidelines for Prevention of Stroke in Patients with Ischemic Stroke or Transient Ischemic Attack: A Statement for Healthcare Professionals from the American Heart Association/American Stroke Association Council on Stroke: Co-Sponsored by the Council on Cardiovascular Radiology and Intervention: The American Academy of Neurology Affirms the Value of This Guideline." [In eng]. Stroke 37, no. 2 (Feb 2006): 577-617.
- Saposnik, G., J. Fang, M. K. Kapral, J. V. Tu, M. Mamdani, P. Austin, S. C. Johnston, Network Investigators of the Registry of the Canadian Stroke, and Group Stroke Outcomes Research Canada Working. "The Iscore Predicts Effectiveness of Thrombolytic Therapy for Acute Ischemic Stroke." [In eng]. Stroke 43, no. 5 (May 2012): 1315-22.
- "Tissue Plasminogen Activator for Acute Ischemic Stroke. The National Institute of Neurological Disorders and Stroke Rt-Pa Stroke Study Group." [In eng]. N Engl J Med 333, no. 24 (Dec 14 1995): 1581-7.
- Wardlaw, J. M., V. Murray, E. Berge, and G. J. Del Zoppo. "Thrombolysis for Acute Ischaemic Stroke." [In eng]. Cochrane Database Syst Rev, no. 4 (2009): CD000213.
- U.S. Drug and Food Administration. (2015). “Label-Alteplase-Food and Drug.”
CPT® only copyright 2022 American Medical Association. All rights reserved. CPT® is a registered trademark of the American Medical Association.
You, your employees and agents are authorized to use CPT® only as contained in The Joint Commission performance measures solely for your own personal use in directly participating in healthcare programs administered by The Joint Commission. You acknowledge that the American Medical Association (“AMA”) holds all copyright, trademark and other rights in CPT®.
Any use not authorized herein is prohibited, including by way of illustration and not by way of limitation, making copies of CPT® for resale and/or license, transferring copies of CPT® to any party not bound by this Agreement, creating any modified or derivative work of CPT®, or making any commercial use of CPT®. License to use CPT® for any use not authorized herein must be obtained through the American Medical Association, Intellectual Property Services, AMA Plaza, 330 North Wabash Avenue, Suite 39300, Chicago, Illinois 60611-5885. Applications are available at the American Medical Association Web site, www.ama- assn.org/go/cpt.
U.S. Government Rights This product includes CPT® which is commercial technical data, which was developed exclusively at private expense by the American Medical Association, 330 North Wabash Avenue, Chicago, Illinois 60611. The American Medical Association does not agree to license CPT® to the Federal Government based on the license in FAR 52.227-14 (Data Rights - General) and DFARS 252.227-7015 (Technical Data - Commercial Items) or any other license provision. The American Medical Association reserves all rights to approve any license with any Federal agency.
Disclaimer of Warranties and Liabilities. CPT® is provided “as is” without warranty of any kind, either expressed or implied, including but not limited to the implied warranties of merchantability and fitness for a particular purpose. Fee schedules, relative value units, conversion factors and/or related components are not assigned by the AMA, are not part of CPT®, and the (AMA is not recommending their use. The AMA does not directly or indirectly practice medicine or dispense medical services. The responsibility for the content of this product is with The Joint Commission, and no endorsement by the AMA is intended or implied. The AMA disclaims responsibility for any consequences or liability attributable to or related to any use, non-use, or interpretation of information contained or not contained in this product.
This Agreement will terminate upon notice if you violate its terms. The AMA is a third party beneficiary to this Agreement.
Should the foregoing terms and conditions be acceptable to you, please indicate your agreement and acceptance by clicking below on the button labeled “accept”.