Measure Information Form
Version 2021B2
Measure Information Form
| Set Measure ID | Performance Measure Name |
|---|---|
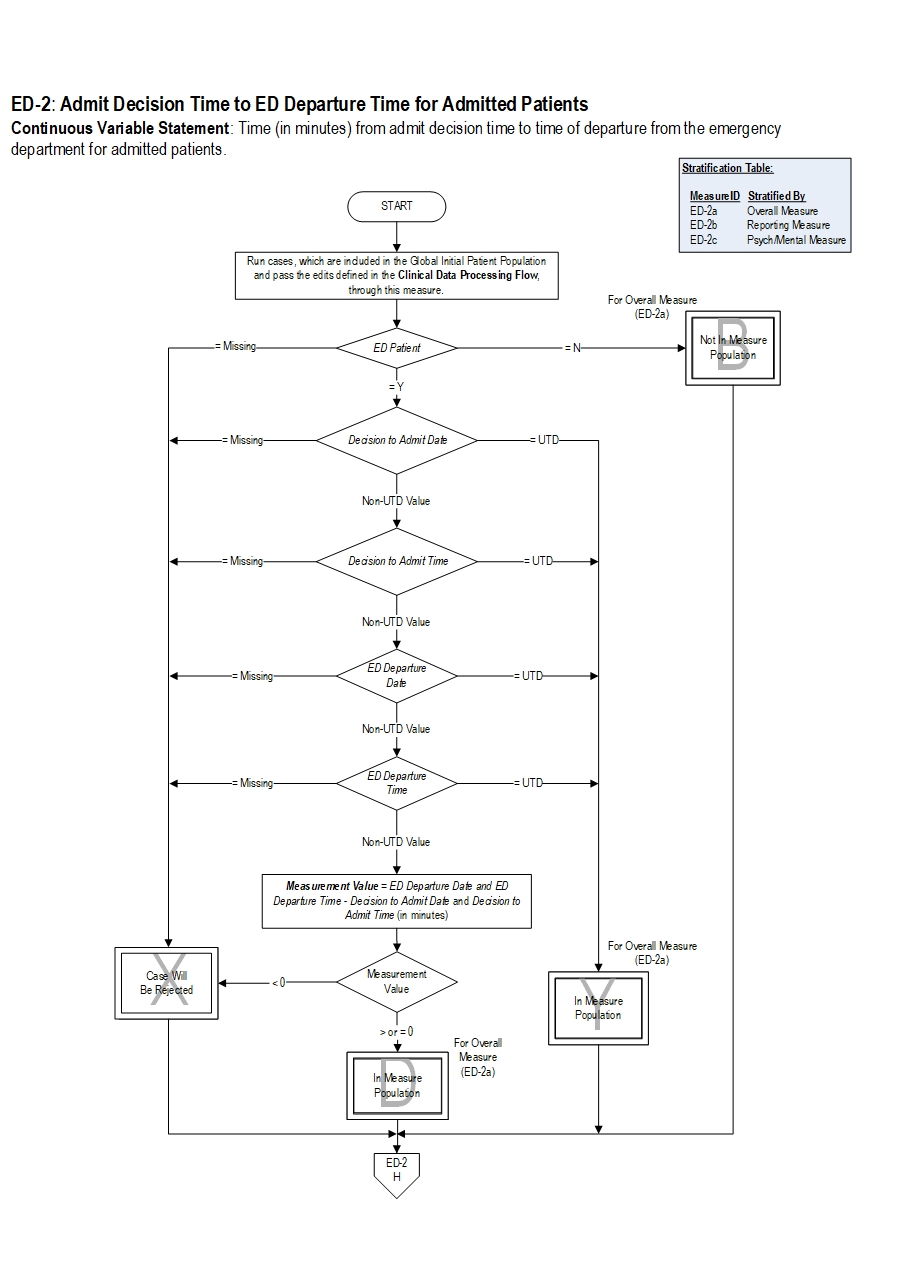
| ED-2a |
Admit Decision Time to ED Departure Time for Admitted Patients – Overall Rate |
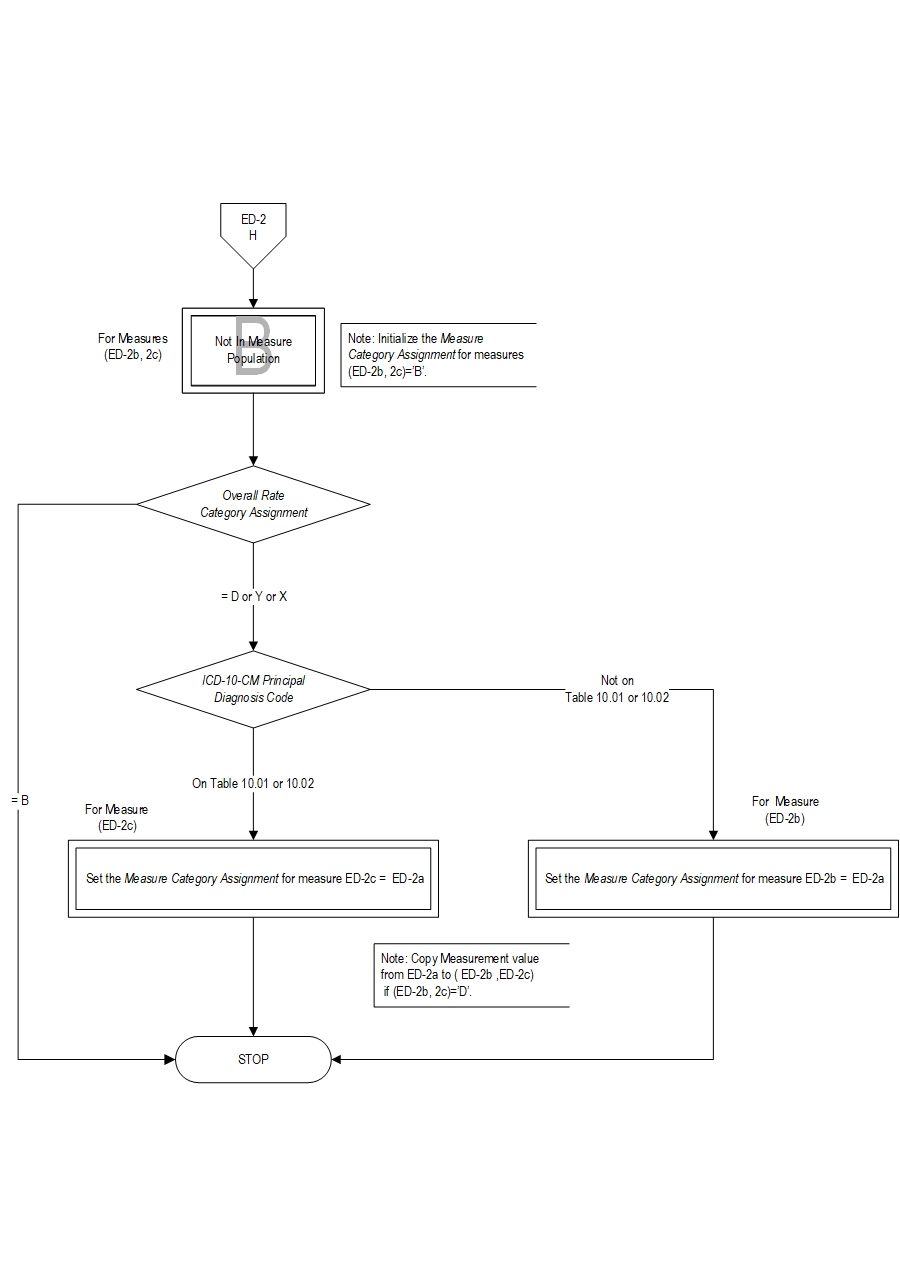
| ED-2b |
Admit Decision Time to ED Departure Time for Admitted Patients – Reporting Measure |
| ED-2c |
Admit Decision Time to ED Departure Time for Admitted Patients –Psychiatric/Mental Health Patients |
Included Populations: Any ED Patient from the facility’s emergency department Excluded Populations: Patients who are not an ED Patient Data Elements:
- Derlet RW, Richards JR. Emergency department overcrowding in Florida,New York, and Texas. South Med J. 2002;95:846-9.
- Derlet RW, Richards JR. Overcrowding in the nation's emergency departments:complex causes and disturbing effects. Ann Emerg Med. 2000;35:63-8.
- Diercks DB, et al. Prolonged emergency department stays of non-ST-segment-elevation myocardial infarction patients are associated with worse adherence to the American College of Cardiology/American Heart Association guidelines for management and increased adverse events. Ann Emerg Med. 2007;50:489-96.
- Fatovich DM, Hirsch RL. Entry overload, emergency department overcrowding,and ambulance bypass. Emerg Med J. 2003;20:406-9.
- Hwang U, Richardson LD, Sonuyi TO, Morrison RS. The effect of emergency department crowding on the management of pain in older adults with hip fracture.J Am Geriatr Soc. 2006;54:270-5.
- Institute of Medicine of the National Academies. Future of emergency care:Hospital-based emergency care at the breaking point. The National Academies Press 2006.
- Institute of Medicine. IOM Report: the future of emergency care in the United States health system. Acad Emer Med. 2006;13(10):1081-5.
- Krochmal P, Riley TA. Increased health care costs associated with ED overcrowding. Am J Emerg Med. 1994;12:265-6.
- Kyriacou DN, Ricketts V, Dyne PL,McCollough MD, Talan DA. A 5-year time study analysis of emergency department patient care efficiency. Ann Emerg Med.1999;34:326-35.
- Nawar ED, Niska RW, Xu J. National Hospital Ambulatory Medical Care Survey:2005 emergency department summary. Adv Data. 2007; (386):1-32.
- Richardson DB. Increase in patient mortality at 10 days associated with emergency department overcrowding. Med J Aust. 2006;184:213-6.
- Sprivulis PC, et al. The association between hospital overcrowding and mortality among patients admitted via Western Australian emergency departments. Med JAust. 2006;184:208-12.
- Trzeciak S, Rivers EP. Emergency department overcrowding in the United States: an emerging threat to patient safety and public health. Emerg Med J.2003;20:402-5.
- United States General Accounting Office GAO. Hospital Emergency Departments: crowded conditions vary among hospitals and communities. 2003;GAO-03-460.
- Wilper AP, Woolhandler S, Lasser KE, McCormick D, Cutrona SL, Bor DH,Himmelstein DU. Waits to see an emergency department physician: U.S. trends and predictors, 1997-2004. Health Aff (Millwood). 2008;27:w84-95.
CPT® only copyright 2019 American Medical Association. All rights reserved. CPT® is a registered trademark of the American Medical Association.
You, your employees and agents are authorized to use CPT® only as contained in The Joint Commission performance measures solely for your own personal use in directly participating in healthcare programs administered by The Joint Commission. You acknowledge that the American Medical Association (“AMA”) holds all copyright, trademark and other rights in CPT®.
Any use not authorized herein is prohibited, including by way of illustration and not by way of limitation, making copies of CPT® for resale and/or license, transferring copies of CPT® to any party not bound by this Agreement, creating any modified or derivative work of CPT®, or making any commercial use of CPT®. License to use CPT® for any use not authorized herein must be obtained through the American Medical Association, Intellectual Property Services, AMA Plaza, 330 North Wabash Avenue, Suite 39300, Chicago, Illinois 60611-5885. Applications are available at the American Medical Association Web site, www.ama- assn.org/go/cpt.
U.S. Government Rights This product includes CPT® which is commercial technical data, which was developed exclusively at private expense by the American Medical Association, 330 North Wabash Avenue, Chicago, Illinois 60611. The American Medical Association does not agree to license CPT® to the Federal Government based on the license in FAR 52.227-14 (Data Rights - General) and DFARS 252.227-7015 (Technical Data - Commercial Items) or any other license provision. The American Medical Association reserves all rights to approve any license with any Federal agency.
Disclaimer of Warranties and Liabilities. CPT® is provided “as is” without warranty of any kind, either expressed or implied, including but not limited to the implied warranties of merchantability and fitness for a particular purpose. Fee schedules, relative value units, conversion factors and/or related components are not assigned by the AMA, are not part of CPT®, and the (AMA is not recommending their use. The AMA does not directly or indirectly practice medicine or dispense medical services. The responsibility for the content of this product is with The Joint Commission, and no endorsement by the AMA is intended or implied. The AMA disclaims responsibility for any consequences or liability attributable to or related to any use, non-use, or interpretation of information contained or not contained in this product.
This Agreement will terminate upon notice if you violate its terms. The AMA is a third party beneficiary to this Agreement.
Should the foregoing terms and conditions be acceptable to you, please indicate your agreement and acceptance by clicking below on the button labeled “accept”.