Measure Information Form
Version 2021B
Measure Information Form
Hyperkalemia is a major risk of aldosterone antagonist therapy. Potassium supplements should be discontinued after the initiation of therapy, and patients should be counseled to avoid high-potassium foods.
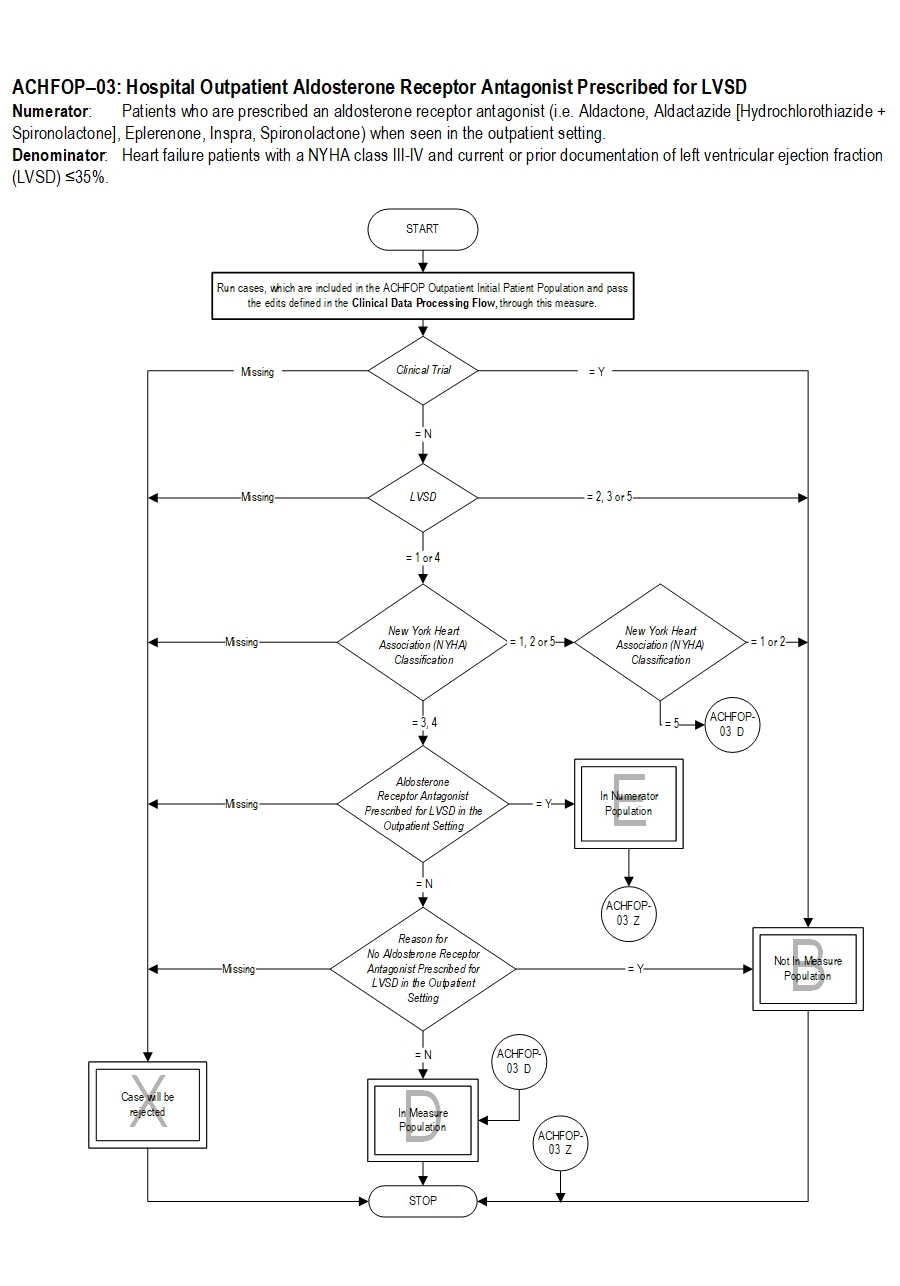
Type Of Measure: Process Improvement Noted As: Increase in the rateIncluded Populations: Not applicable Excluded Populations: None Data Elements:Denominator Statement: Heart failure patients with a NYHA class III-IV and current or prior documentation of left ventricular ejection fraction (LVSD) ≤35%.
Included Populations:Excluded Populations:
- E/M Code for hospital outpatient encounter as defined in Appendix A, Table 2.0
- An ICD-10-CM Principal Diagnosis Code for HF as defined in Appendix A, Table 2.1, and
- Documentation of LVSD ≤35%
- New York Heart Association (NYHA) Functional Classification III-IV
Data Elements:
- Clinical Trial
- Patients who had a left ventricular assistive device (LVAD) or heart transplant procedure during the hospital stay or a past medical history of an LVAD or heart transplant (ICD-10-PCS procedure code for LVAD and heart transplant as defined in Appendix A Table 2.2, and ICD-10 diagnosis codes on Table 2.13)
- Patients less than 18 years of age
- Patients with a documented Reason for No Aldosterone Receptor Antagonist Prescribed for LVSD in the Outpatient Setting
- Birthdate
- Clinical Trial
- Discharge Code
- E/M Code
- ICD-10-CM Principal Diagnosis Code
- ICD-10-PCS Other Procedure Codes
- ICD-10-PCS Principal Procedure Code
- ICD-10-PCS Principal Procedure Date
- LVSD
- New York Heart Association (NYHA) Classification
- Outpatient Encounter Date
- Reason for No Aldosterone Receptor Antagonist Prescribed in the Outpatient Setting
- Hunt SA, Abraham WT, Chin MH, Felman AM, Francis GS, Ganiats TG, Jessup M, Konstam MA, Mancini DM, Michl K, Oates JA, Rahko PS, Silver MA, Stevenson LW, Yancy CW. 2009 Focused update incorporated Into the ACC/AHA 2005 guidelines for the diagnosis and management of heart failure in adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines Developed in Collaboration With the International Society for Heart and Lung Transplantation. Circulation. 2009;119(14):e391-e479.
- Lindenfeld J, Albert NM, Boehmer JP, Collins SP, Ezekowitz JA, Givertz MM, Klapholz M, MoserDK, Rogers JG, Starling RC, Stevenson WG, Tang WHW, Teerlink JR, Walsh MN. Executive Summary: HFSA 2010 Comphrensive Heart Failure Practice Guideline. J Card Fail 2010;16:475-539.
- Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE Jr, Drazner MH, Fonarow GC, Geraci SA, Horwich T, Januzzi JL, Johnson MR, Kasper EK, Levy WC, Masoudi FA, McBride PE, McMurray JJV, Mitchell JE, Peterson PN, Riegel B, Sam F, Stevenson LW, Tang WHW, Tsai EJ, Wilkoff BL. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;128:e240–e327.
CPT® only copyright 2019 American Medical Association. All rights reserved. CPT® is a registered trademark of the American Medical Association.
You, your employees and agents are authorized to use CPT® only as contained in The Joint Commission performance measures solely for your own personal use in directly participating in healthcare programs administered by The Joint Commission. You acknowledge that the American Medical Association (“AMA”) holds all copyright, trademark and other rights in CPT®.
Any use not authorized herein is prohibited, including by way of illustration and not by way of limitation, making copies of CPT® for resale and/or license, transferring copies of CPT® to any party not bound by this Agreement, creating any modified or derivative work of CPT®, or making any commercial use of CPT®. License to use CPT® for any use not authorized herein must be obtained through the American Medical Association, Intellectual Property Services, AMA Plaza, 330 North Wabash Avenue, Suite 39300, Chicago, Illinois 60611-5885. Applications are available at the American Medical Association Web site, www.ama- assn.org/go/cpt.
U.S. Government Rights This product includes CPT® which is commercial technical data, which was developed exclusively at private expense by the American Medical Association, 330 North Wabash Avenue, Chicago, Illinois 60611. The American Medical Association does not agree to license CPT® to the Federal Government based on the license in FAR 52.227-14 (Data Rights - General) and DFARS 252.227-7015 (Technical Data - Commercial Items) or any other license provision. The American Medical Association reserves all rights to approve any license with any Federal agency.
Disclaimer of Warranties and Liabilities. CPT® is provided “as is” without warranty of any kind, either expressed or implied, including but not limited to the implied warranties of merchantability and fitness for a particular purpose. Fee schedules, relative value units, conversion factors and/or related components are not assigned by the AMA, are not part of CPT®, and the (AMA is not recommending their use. The AMA does not directly or indirectly practice medicine or dispense medical services. The responsibility for the content of this product is with The Joint Commission, and no endorsement by the AMA is intended or implied. The AMA disclaims responsibility for any consequences or liability attributable to or related to any use, non-use, or interpretation of information contained or not contained in this product.
This Agreement will terminate upon notice if you violate its terms. The AMA is a third party beneficiary to this Agreement.
Should the foregoing terms and conditions be acceptable to you, please indicate your agreement and acceptance by clicking below on the button labeled “accept”.