Measure Information Form
Version 2021A
Measure Information Form
- Diagnosis of a myocardial infarction (MI)
- Coronary artery bypass graft (CABG) surgery
- Percutaneous coronary intervention (PCI)
- Cardiac valve repair/replacement
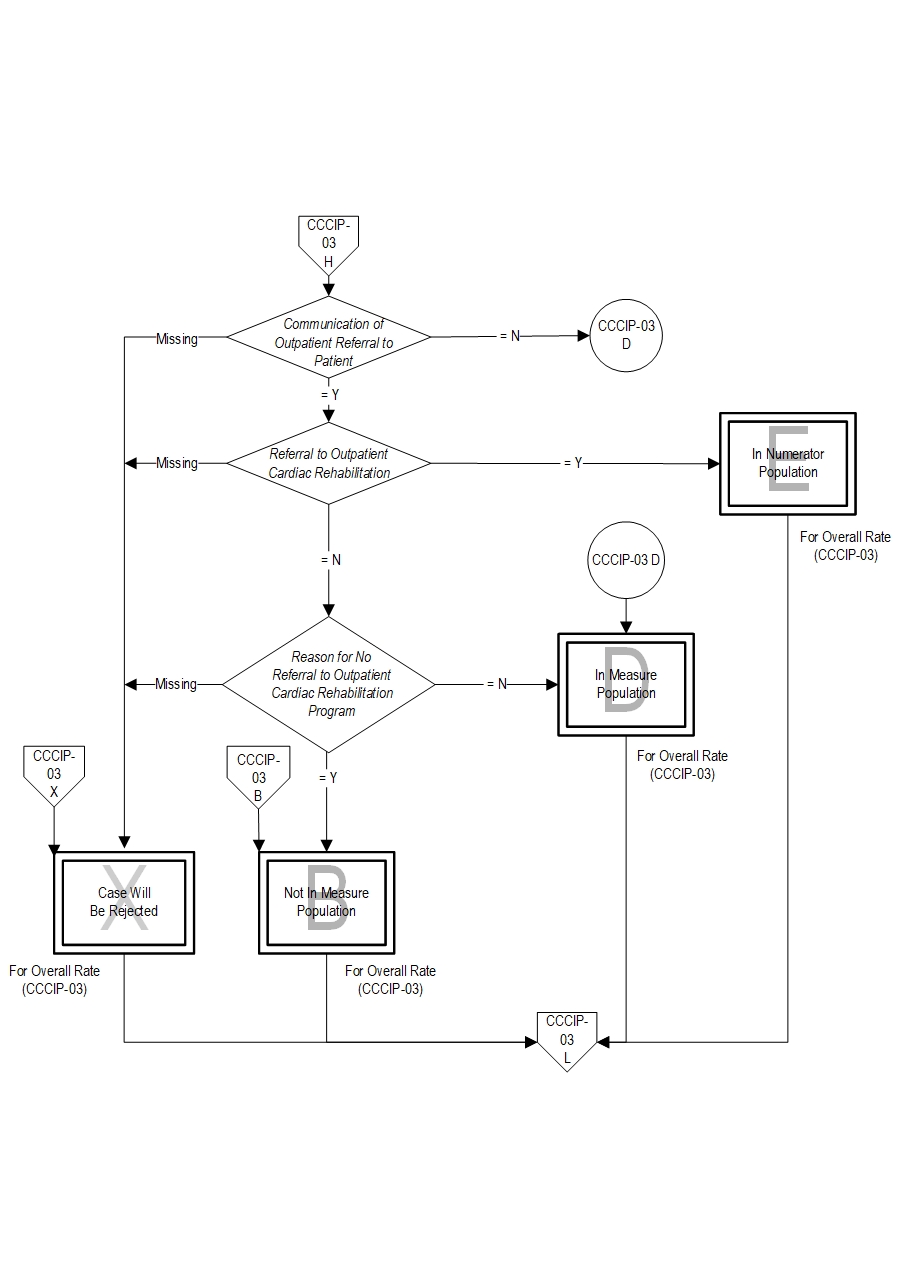
- Communication between the healthcare provider and the patient of the recommendation to attend an outpatient cardiac rehabilitation program AND referral sent to outpatient cardiac rehabilitation program
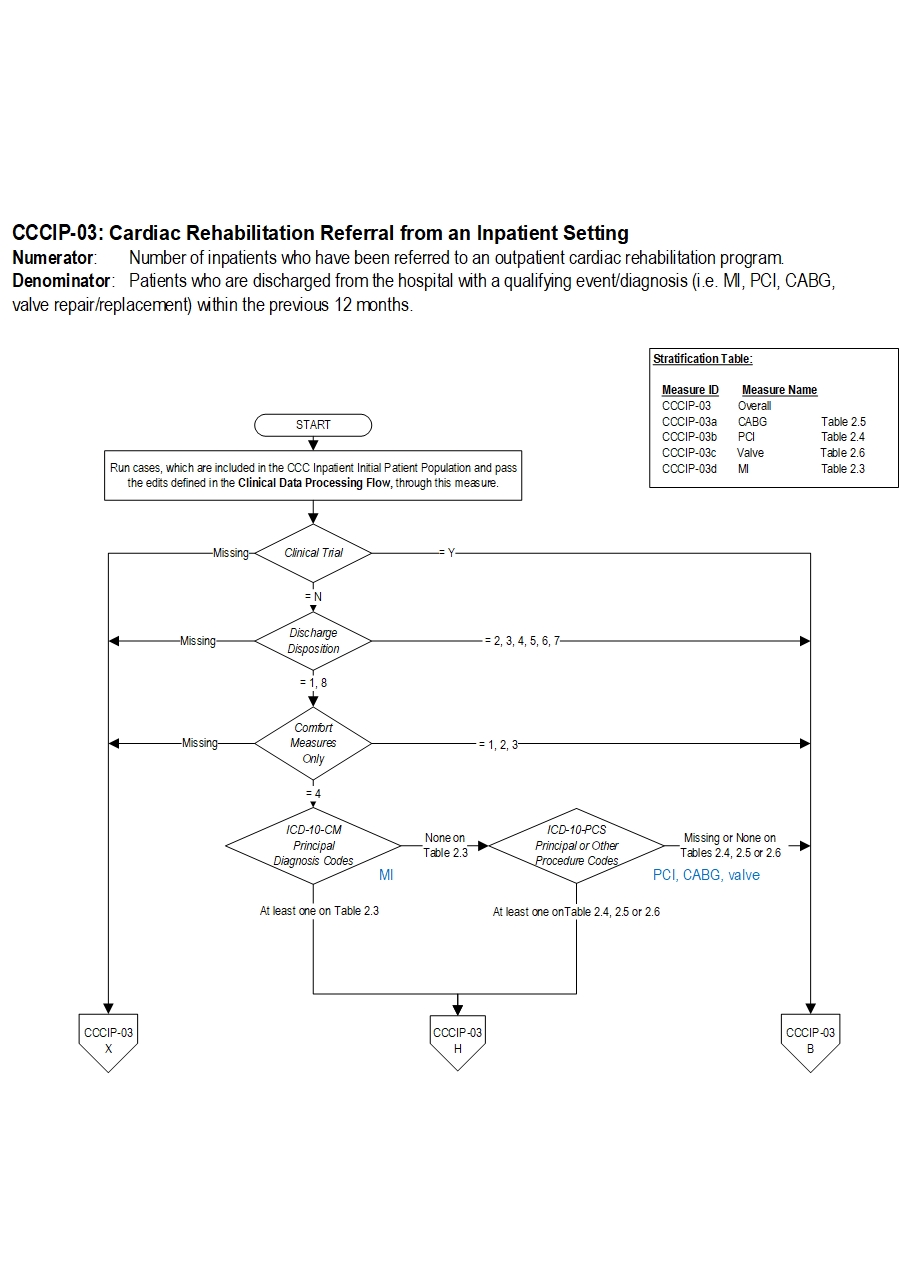
Included Populations: Not applicable Excluded Populations: Not applicable Data Elements:Denominator Statement: Patients who are discharged from the hospital with a qualifying event/diagnosis (i.e. MI, PCI, CABG, valve repair/replacement).
Included Populations:Excluded Populations:
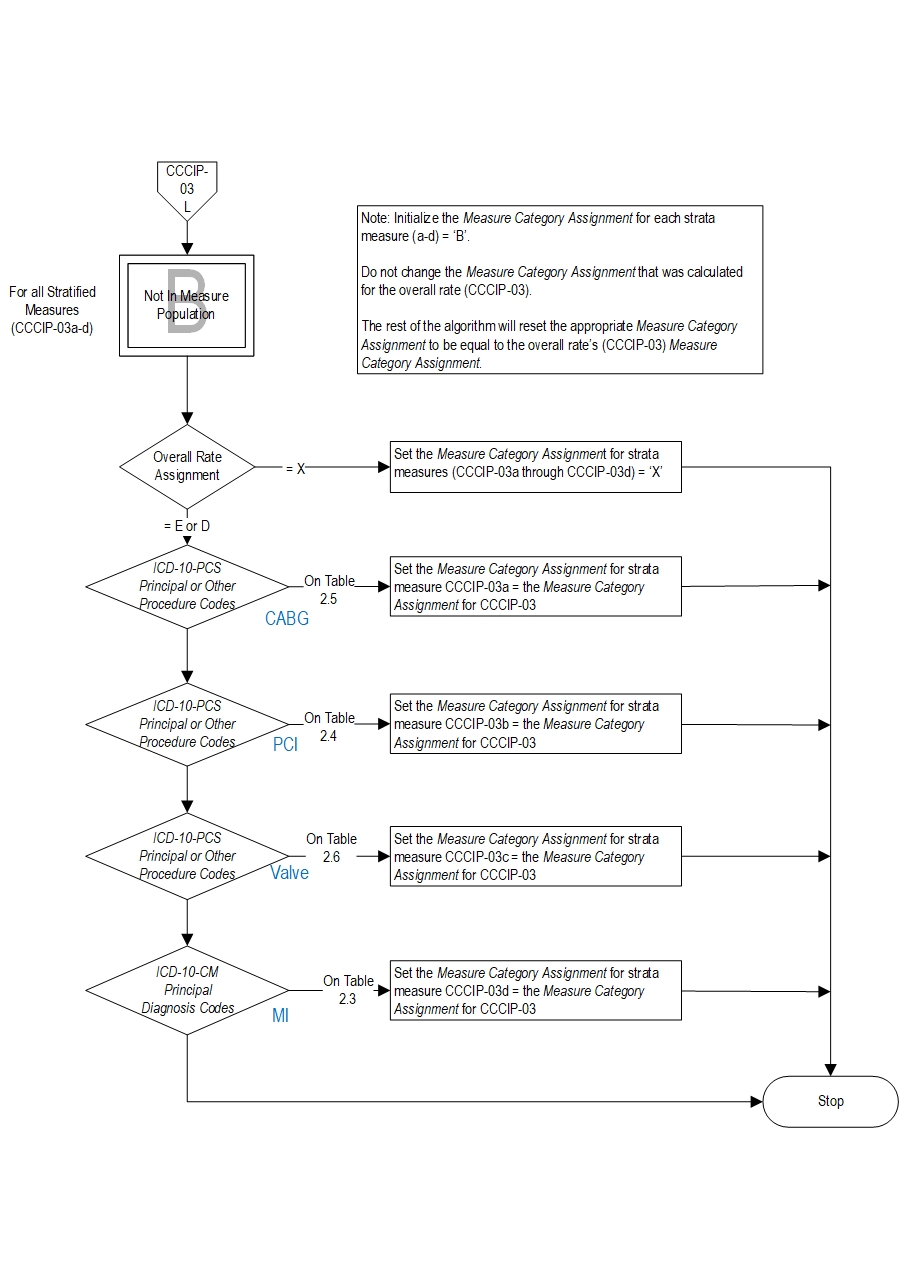
- Patients with a ICD-10-CM Principal Diagnosis Code for MI as defined in Appendix A, Table 2.3.
- Patients with an ICD-10-PCS Principal or Other Procedure Code for PCI as defined in Appendix A, Table 2.4.
- Patients with an ICD-10-PCS Principal or Other Procedure Code for CABG as defined in Appendix A, Table 2.5.
- Patients with an ICD-10-PCS Principal or Other Procedure Code for valve repair/replacement as defined in Appendix A, Table 2.6.
Data Elements:
- Patients less than 18 years of age
- Patients with a documented Reason for No Referral to Outpatient Cardiac Rehabilitation Program
- Patients who expired
- Patients who left against medical advice (AMA)
- Patients discharged to another hospital
- Patients discharged to another healthcare facility
- Patients discharged to home for hospice care
- Patients discharged to a healthcare facility for hospice care
- Patients who have a Length of Stay greater than 120 days
- Patients enrolled in a Clinical Trial
- Patients with Comfort Measures Only documented
- Patients who had a left ventricular assist device (LVAD) or heart transplant procedure (ICD-10-PCS Procedure Code for LVAD or heart transplant as defined in Appendix A, Table 2.2 or Table 2.13)
- Admission Date
- Birthdate
- Clinical Trial
- Comfort Measures Only
- Discharge Date
- Discharge Disposition
- ICD-10-CM Other Diagnosis Codes
- ICD-10-CM Principal Diagnosis Code
- ICD-10-PCS Other Procedure Codes
- ICD-10-PCS Other Procedure Dates
- ICD-10-PCS Principal Procedure Code
- ICD-10-PCS Principal Procedure Date
- Reason for No Referral to Outpatient Cardiac Rehabilitation Program
- Ades, P., Keteyian, S., Wright, J., Hamm, L., Lui, K., Newlin, K., et al. (2017). Increasing Cardiac Rehabilitation Participation From 20% to 70%: A Road Map From the Million Hearts Cardiac Rehabilitation Collaborative. Mayo Clin Proc. Feb; 92(2): 234-242.
- American Heart Association. (2018). Cardiac Rehab 101. Retrieved April 27, 2018 at: http://www.heart.org/HEARTORG/Conditions/More/CardiacRehab/What-is-Cardiac-Rehabilitation_UCM_307049_Article.jsp#.WuNs0C7waUl
- Amsterdam EA, Wenger NK, Brindis RG, et al. (2014). AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 64:e139–228.
- Beatty, A., Bradley, S., Maynard, C., McCabe, J., (2017). Referral to Cardiac Rehabilitation After Percutaneous Coronary Intervention, Coronary Artery Bypass Surgery, and Valve Surgery Data From the Clinical Outcomes Assessment Program. Circ Cardiovasc Qual Outcomes. 10:e003364.
- Hillis LD, Smith PK, Anderson JL, et al. (2011). 2011 ACCF/AHA guideline for coronary artery bypass graft surgery. a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Developed in collaboration with the American Association for Thoracic Surgery, Society of Cardiovascular Anesthesiologists, and Society of Thoracic Surgeons. J Am Coll Cardiol. 58:e123–210.
- Levine GN, Bates ER, Blankenship JC, et al. (2011). 2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention: a report of the American College of CardiologyFoundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. J Am Coll Cardiol. 58:e44–122.
- O’Gara PT, Kushner FG, Ascheim DD, et al. (2013). ACCF/AHA guideline for the management of ST elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;61:e78–140.
- Smith SC Jr., Benjamin EJ, Bonow RO, et al. (2011). AHA/ACCF secondary prevention and risk reduction therapy for patients with coronary and other atherosclerotic vascular disease: 2011 update: a guideline from the American Heart Association and American College of Cardiology Foundation. J Am Coll Cardiol. 58:2432–46.
- Thomas, R., Balady, G., Banka, G., Beckie, T., Chiu, J., Gokak, S. (2018). 2018 ACC/AHA Clinical Performance and Quality Measures for Cardiac Rehabiliation. Circ Cardiovasc Qual Outcomes. 2018 Apr;11(4):e000037.
CPT® only copyright 2019 American Medical Association. All rights reserved. CPT® is a registered trademark of the American Medical Association.
You, your employees and agents are authorized to use CPT® only as contained in The Joint Commission performance measures solely for your own personal use in directly participating in healthcare programs administered by The Joint Commission. You acknowledge that the American Medical Association (“AMA”) holds all copyright, trademark and other rights in CPT®.
Any use not authorized herein is prohibited, including by way of illustration and not by way of limitation, making copies of CPT® for resale and/or license, transferring copies of CPT® to any party not bound by this Agreement, creating any modified or derivative work of CPT®, or making any commercial use of CPT®. License to use CPT® for any use not authorized herein must be obtained through the American Medical Association, Intellectual Property Services, AMA Plaza, 330 North Wabash Avenue, Suite 39300, Chicago, Illinois 60611-5885. Applications are available at the American Medical Association Web site, www.ama- assn.org/go/cpt.
U.S. Government Rights This product includes CPT® which is commercial technical data, which was developed exclusively at private expense by the American Medical Association, 330 North Wabash Avenue, Chicago, Illinois 60611. The American Medical Association does not agree to license CPT® to the Federal Government based on the license in FAR 52.227-14 (Data Rights - General) and DFARS 252.227-7015 (Technical Data - Commercial Items) or any other license provision. The American Medical Association reserves all rights to approve any license with any Federal agency.
Disclaimer of Warranties and Liabilities. CPT® is provided “as is” without warranty of any kind, either expressed or implied, including but not limited to the implied warranties of merchantability and fitness for a particular purpose. Fee schedules, relative value units, conversion factors and/or related components are not assigned by the AMA, are not part of CPT®, and the (AMA is not recommending their use. The AMA does not directly or indirectly practice medicine or dispense medical services. The responsibility for the content of this product is with The Joint Commission, and no endorsement by the AMA is intended or implied. The AMA disclaims responsibility for any consequences or liability attributable to or related to any use, non-use, or interpretation of information contained or not contained in this product.
This Agreement will terminate upon notice if you violate its terms. The AMA is a third party beneficiary to this Agreement.
Should the foregoing terms and conditions be acceptable to you, please indicate your agreement and acceptance by clicking below on the button labeled “accept”.