Release Notes:
Measure Information Form
Version 2018A
Measure Information Form
Version 2018A
Measure Information Form
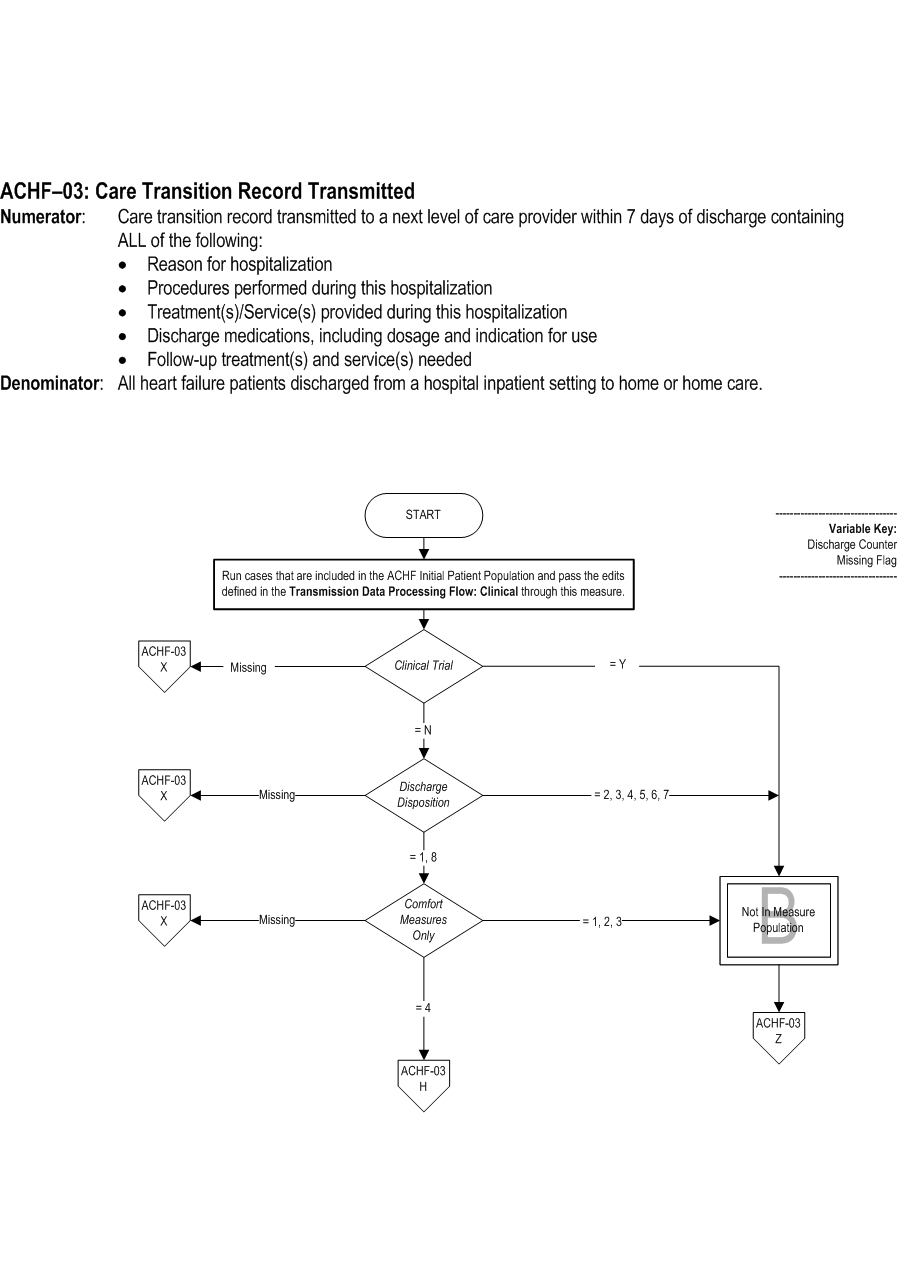
- Reason for hospitalization
- Procedures performed during this hospitalization
- Treatment(s)/Service(s) provided during this hospitalization
- Discharge medications, including dosage and indication for use
- Follow-up treatment and services needed (e.g., post-discharge therapy, oxygen therapy, durable medical equipment)
- The program identifies an individual to coordinate the care of participants.
- The program provides participants with access to a practitioner 24 hours a day, 7 days a week (access may include use of the telephone and the internet, and referral to urgent care settings).
- The program communicates important information regarding co-occurring conditions and co-morbidities to appropriate practitioner(s) to treat or manage conditions.
- The program care coordinator(s) is responsible for the communication of relevant information among practitioners and across settings.
- The program care coordinator(s) is responsible for sharing information among practitioners in a timeframe that meets the participant's needs.
- The program care coordinator(s) is responsible for confirming practitioner receipt of information and actions taken.
Numerator Statement: Care transition record transmitted to a next level of care provider within 7 days of discharge containing ALL of the following:
Risk Adjustment: No.
Data Collection Approach: Retrospective data sources for required data elements include administrative data and medical records.
Data Accuracy: Variation may exist in the assignment of ICD-10 codes; therefore, coding practices may require evaluation to ensure consistency.
Measure Analysis Suggestions: None
Sampling: Yes. Please refer to the measure set specific sampling requirements and for additional information see the Population and Sampling Specifications section.
Data Reported As: Aggregate rate generated from count data reported as a proportion. Aggregate rate generated from count data reported as a proportion
Selected References: - Reason for hospitalization
- Procedures performed during this hospitalization
- Treatment(s)/Service(s) provided during this hospitalization
- Discharge medications, including dosage and indication for use
- Follow-up treatment(s) and service(s) needed
Included Populations: Not applicable Excluded Populations: None Data Elements:Denominator Statement: All heart failure patients discharged from a hospital inpatient setting to home or home care
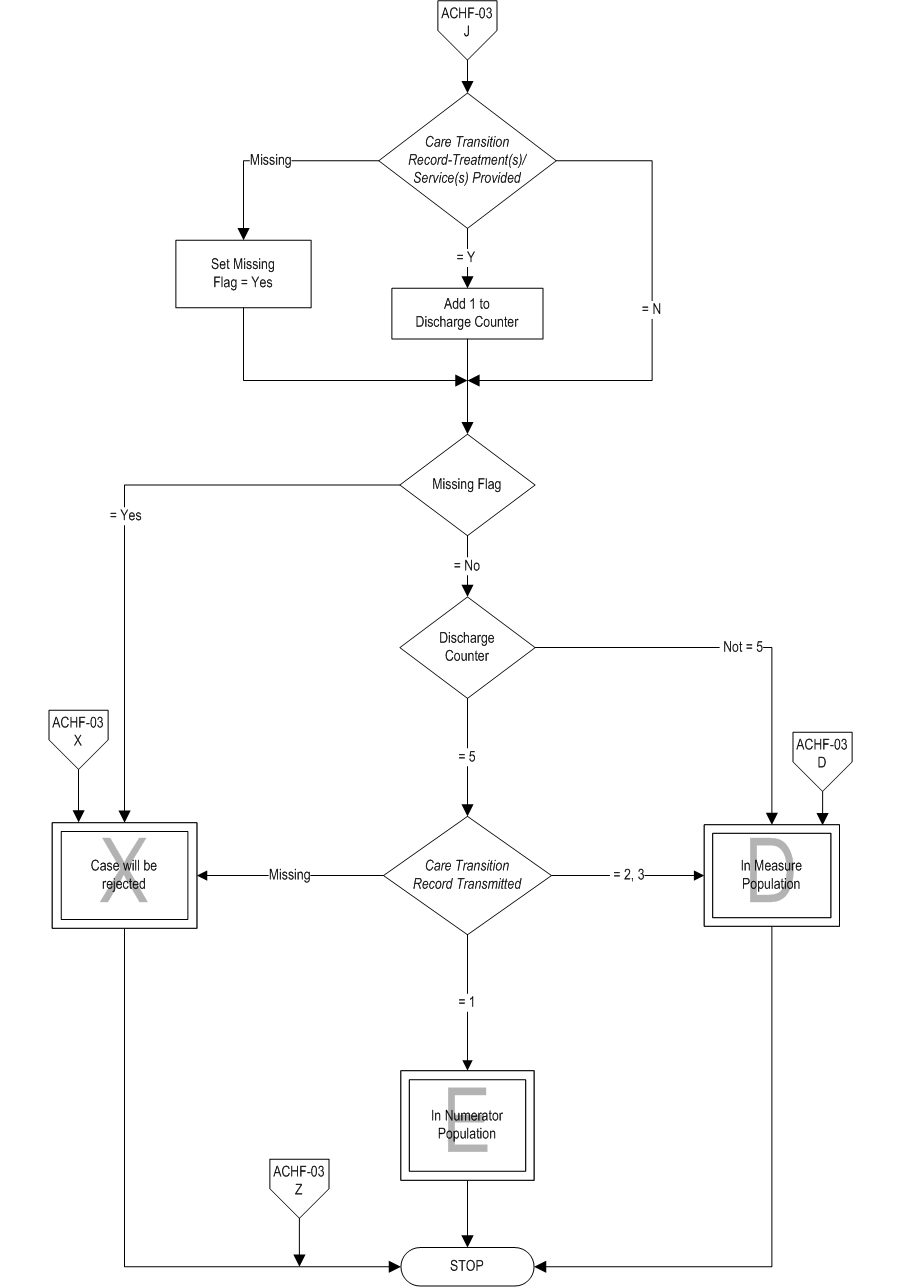
- Care Transition Record Transmitted
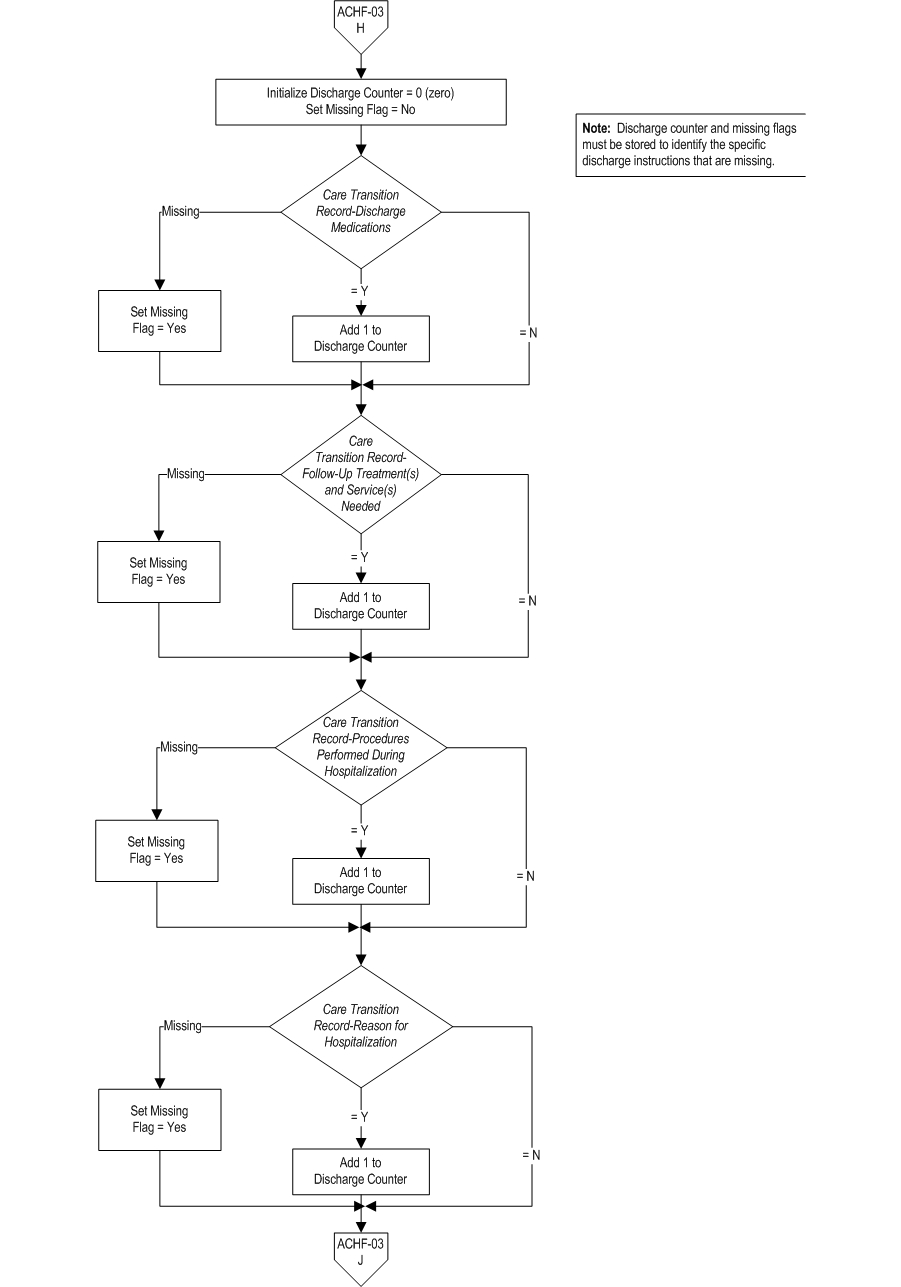
- Care Transition Record-Discharge Medications
- Care Transition Record-Follow-Up Treatment(s) and Service(s) Needed
- Care Transition Record-Procedures Performed During Hospitalization
- Care Transition Record-Reason for Hospitalization
- Care Transition Record-Treatment(s)/Service(s) Provided
Included Populations:Excluded Populations:
- Discharges with ICD-10-CM Principal Diagnosis Code for HF as defined in Appendix A, Table 2.1, and
- A discharge to home, home care, or court/law enforcement
Data Elements:
- Patients who had a left ventricular assistive device (LVAD) or heart transplant procedure during hospital stay (ICD-10-PCS procedure code for LVAD and heart transplant as defined in Appendix A, Table 2.2)
- Patients less than 18 years of age
- Patient who have a Length of Stay greater than 120 days
- Patients with Comfort Measures Only documented
- Patients enrolled in a Clinical Trial
- Patients discharged to locations other than home, home care, or law enforcement
- Patients who left against medical advice (AMA)
- Bell CM, Schnipper JL, Auerback AD, Kaboli PJ, Wetterneck TB, Gonzales DV, Arora VM, Zhang JX, Meltzer DO; Association of communication between hospital-based physicians and Primary care providers with patient outcomes. J Gen Intern Med. 2008; 24(3):381-386.
- Bodenheimer T. Coordinating care â“ a perilous journey through the health care system.NEJM. 2008;358(10): 1064-1071.
- Kripalani S, Applications/LocalApps.LeFevre F, Phillips CO, et al. Deficits in communication and information transfer between hospital-based and primary care physicians: Implications for patient safety and continuity of care. JAMA. 2007; 297(8):831-841.
- Ravel AN, Marchiori GE, Arnold JMO. Improving the continuity of care following discharge of patients hospitalized with heart failure: Is the discharge summary adequate? Can J Cardiol. 2003;19(4):365-370.
- van Walraven C, Seth R, Austin PC, Laupacis A. Effect of discharge summary availability during post-discharge visits on hospital readmission. J Gen Intern Med. 2002;17(3):186-192.
- The Joint Commission. The Joint Commission's 2017 Comprehensive Certification Manual for Disease-Specific Care: Advanced Certification in Heart Failure Addendum. Oakbrook Terrace, IL: Author. 2017.
| Related Topics |
Questions? Ask Question to Joint Commission staff
Copyright © 2018 by The Joint Commission.